-
 Fill
the form below
Fill
the form below
Fill
the form below

Vesicoureteric reflux is a common problem in children with urinary infections. Surgical correction is possible in the few who will require treatment.
Vesicoureteric reflux (VUR) is a condition, commonly detected during the investigation of urinary tract infection (UTI) in children, in which urine can flow back from the bladder toward the kidneys.
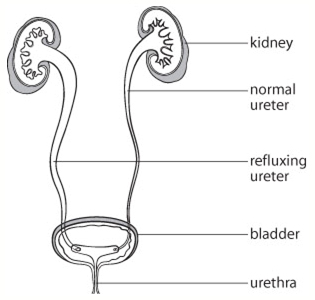
Urine produced by the kidneys drains down tubes (the ureters) into the bladder where it is stored until it is appropriate to empty through the urethra (“urine passage”). Normally, one-way “flap valves” at the junction between the ureters and the bladder prevent the backflow of urine toward the kidneys.
When these valves do not develop properly, backwash of urine from the bladder to the ureter and kidney, vesicoureteric reflux, can occur. One or both kidneys may be involved from the time of birth. Usually, VUR alone will produce no symptoms or cause any harm. Should a child develop a bladder infection, however, the infected urine flowing back to the kidney(s) can cause a kidney infection. This can make the child quite ill with fever and chills, and, may result in permanent scarring of the kidney. In most cases urinary infection does not cause VUR, nor does VUR cause urinary infection.

Underlying urinary tract abnormalities are common in children with urinary infections. A child who experiences a UTI may undergo imaging studies to demonstrate urinary tract anatomy and determine the presence of VUR.
The kidneys may be examined by ultrasound, a painless test without x-ray exposure. The identification of VUR requires another test, the voiding cysto-urethrogram (VCUG). A small tube (catheter) is inserted into the child’s bladder through the urethra. The bladder is then filled with contrast material (“dye”) and x-rays are taken as the child voids. The appearance of contrast in the ureter or kidney confirms the suspicion of VUR and its severity can be graded.
A nuclear cystogram is carried out much like a VCUG, but exposes your child to less radiation. A renal nuclear scan can accurately assess kidney function and the presence of scars.
In time, VUR frequently will resolve without treatment as the valves develop in the growing child. Many cases of VUR can be monitored safely without specific treatment as long as infection is prevented. During this period of observation, your doctor may recommend small daily doses of antibiotics in an effort to prevent infection and kidney damage.
The severity (grade) of VUR and a child’s abnormal voiding habits, such as prolonged urine holding, will determine the duration of VUR. A child with VUR should be encouraged to void regularly and constipation should be prevented. Usually, VUR resolves within two years for boys and four years for girls.
we may recommend regular cystograms, usuallyevery 12 to 18 months, and periodic ultrasounds until the VUR has resolved or your child is out of the period of risk.
In some cases, VUR is best corrected with surgery. Surgery is often recommended if a child develops a severe urinary infection while on preventive antibiotics or if preventive antibiotics cannot be taken. Worsening VUR or new kidney scarring demonstrated on follow-up imaging studies may indicate the need for surgery, as may persistent VUR despite an adequate period of observation.
Two surgical approaches are available to correct VUR. The STING procedure involves the injection of an implant under the connection of the ureter to the bladder to strengthen the flap valve. This is done under general anaesthetic (the child is asleep), through a narrow tube (cystoscope) passed through the urethra. No incision is required and your child should be able to return home on the day of surgery. The STING procedure has a high cure rate, but some children require more than one injection.
Ureteric reimplantation is recommended for some children with VUR. A flap valve is created by tunneling the affected ureter through the bladder wall. A general anaesthetic is required and an incision is made in the lower abdomen.
Women who have had VUR as girls often have an increased risk of urinary infections with the onset of sexual activity and pregnancy, even if the VUR has been successfully corrected. Kidney scarring resulting from childhood infections may predispose to high blood pressure in adults. The blood pressure should be monitored regularly in any adult who has had VUR with kidney scarring.
VUR may run in families. Up to two thirds of the children of refluxing parents are born with VUR. About one third of brothers and sisters of children with VUR will also have the problem even if they have never had a UTI. Your doctor can discuss the pros and cons of screening imaging studies for any children at risk of VUR.
VUR is a common problem in children with urinary infections. Most often, it will resolve in time without treatment or serious consequence as long as infection is prevented. Surgery can successfully cure VUR in those children who need treatment.
Bedwetting or nocturnal enuresis is a common problem in children.
The bladder is a hollow organ, which stores urine produced...
Benign prostatic hyperplasia (BPH) is a common condition in aging men...
Erectile Dysfunction is the persistent inability to achieve and maintain...
The kidneys play an important role in eliminating waste products...
Scrotal pain is any discomfort of the scrotum or its contents...
Robotically-assisted surgery was developed to overcome...
connect us on :
